

ChartLogic Team
November 29, 2016



Since our last post, Deciphering the Confusion of MACRA, MIPS & APM, the Quality Payment Program (QPP) final rule was released. There have been several changes that have streamlined and eased the participation for more clinicians to participate. This was even more evident with the early announcement of “pick your pace” by the Acting Director of CMS, Andy Slavitt. You can read Andy’s full blog post about the QPP here.
Before we dive into the Quality category, let’s define who is eligible to participate in the MIPS program.
The former term, Eligible Provider, has now been replaced by Eligible Clinician. An Eligible Clinician (EC) is defined and identified by having a unique billing Tax Identification Number (TIN) and National Provider Identification (NPI) combination used to report. This includes physicians, physician assistants, nurse practitioners, clinical nurse specialists, certified registered nurse anesthetists, and any groups that include these professionals.
A group is defined as a single TIN with two or more MIPS Eligible Clinicians, as identified by their individual NPI, who have reassigned their Medicare billing rights to the TIN. The QPP specifically mentions that those clinicians who participate as a group must meet the definition of a group at all times during the performance period and that all ECs must aggregate their performance data across their TIN. Groups must report all four MIPS performance categories.
However, just like past CMS programs, there is an exception to the rule. Any new Medicare-enrolled ECs during the year and any ECs who bill less than $30,000 or see less than 100 Part-B patients annually are exempt from the MIPS program.
Though MIPS inherits most of its Quality measures from Physician Quality Reporting System (PQRS), the MIPS measures are far less arduous, which CMS intends to capitalize on as they strive to unify the QPP. The final rule aims to merge PQRS reporting measures for the use of CEHRT and QCDRs.
The Quality performance category measures will also be updated annually on or before November 1st each year.
ECs are now required to report on at least six quality measures with at least one being an outcome measure. Unlike the PQRS program where ECs were penalized for not meeting performance levels, ECs are now encouraged to pick the most applicable measures to their practice. Letting physicians decide what is clinically relevant is an effort to increase overall quality reporting.
In 2017, ECs can also pick their pace of participation. To be considered a full participant in MIPS, ECs should report a minimum of a continuous 90-days. Although 90-days is the minimum, ECs can and are encouraged to report the full year. Just like the 2016 reporting year, reporting for the Quality category can be independently reported and does not have to coincide with any other QPP category’s performance reporting period for 2017.
ECs can decide to report on specialty-specific measure sets as an alternative reporting method, if applicable. Below are the possible options under this method:
Part of the Quality category will be a check for data completeness to help ensure accuracy in each ECs quality performance score. This means that an Individual EC or group submitting data using QCDRs, qualified registries, or EHRs must submit data on at least 50% of their patients for both Medicare and non-Medicare patients.
Individual ECs submitting data using Medicare Part B claims would need to report on at least 50% of the Medicare Part B patients. While groups submitting data using the CMS Web Interface or CMS-approved survey vendor to report the CAHPS for the MIPS survey must meet the data submission requirements on the sample of the Medicare Part B patients, which CMS provides.
Below is a summary of all the different submission options and their data completeness.
| Performance Period | Measure Type | Submission Mechanism | Submission Criteria | Data Completeness |
|---|---|---|---|---|
| A minimum of one continuous 90-day period during CY2017 | Individual MIPS eligible clinicians | Part B Claims | Report at least six measures including one outcome measure, or if an outcome measure is not available report another high priority measure; if less than six measures apply then report on each measure that is applicable. MIPS eligible clinicians and groups will have to select their measures from either the list of all MIPS Measures in Table A or a set of specialty-specific measures in Table E | 50 percent of MIPS eligible clinician’s Medicare Part B patients for the performance period. |
| A minimum of one continuous 90-day period during CY2017 | Individual MIPS eligible clinicians or Groups | QCDR Qualified Registry EHR | Report at least six measures including one outcome measure, or if an outcome measure is not available report another high priority measure; if less than six measures apply then report on each measure that is applicable. MIPS eligible clinicians and groups will have to select their measures from either the list of all MIPS Measures in Table A or a set of specialty-specific measures in Table E | 50 percent of MIPS eligible clinician’s or groups patients across all payers for the performance period. |
| Jan 1-Dec 31 | Groups | CMS Web Interface | Report on all measures included in the CMS Web Interface; AND populate data fields for the first 248 consecutively ranked and assigned Medicare beneficiaries in the order in which they appear in the group’s sample for each module/measure. If the pool of eligible assigned beneficiaries is less than 248, then the group would report on 100 percent of assigned beneficiaries | Sampling requirements for their Medicare Part B patients. |
| Jan 1-Dec 31 | Groups | CAHPS for MIPS Survey | CMS-approved survey vendor would have to be paired with another reporting mechanism to ensure the minimum number of measures are reported. CAHPS for MIPS Survey would fulfill the requirement for one patient experience measure towards the MIPS quality data submission criteria. CAHPS for MIPS Survey will only count for one measure | Sampling requirements for their Medicare Part B patients. |
Source: https://www.federalregister.gov/d/2016-25240/p-1494
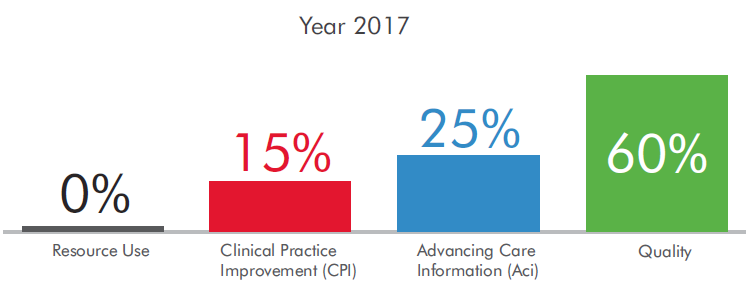
The Quality category in 2017 performance year will end up accounting for 60% of the Composite Performance Score (CPS) which will determine adjustments in the 2019 payment year. After the first payment year, the quality category will be reduced to 50%, and then ultimately to 30% by the performance year 2019.
However, due to 2017 being a transition year for ECs into the QPP, participation in any one measure category for a continuous 90-days will meet the required 3-points to receive a positive payment adjustment.
We suggest reporting at least the minimum six measures for at least a continuous 90-days in 2017 to get the required 3-points that will allow you to receive a positive payment in 2019. This is due to the easy entry into the Quality Payment Program for all Medicare providers that CMS is trying to push for the 2017 transition year.
We also suggest that if you have not started reporting PQRS measures 2017 is the year to begin getting familiar with the requirements data that needs to be recorded. The transition year provides practices and providers the ability to make mistakes during the implementation and learning curve to participate.
ChartLogic is the Ambulatory Division of © 2026 Medsphere Systems Corporation.



